
Podcast: Play in new window | Download (Duration: 23:01 — 21.1MB)
Subscribe: Apple Podcasts | RSS | More
Hi everyone,
Thanks for joining us again, this week I am joined by my colleague Prof Yee Leung, Head of Gynaecological Oncology in Western Australia, to discuss the obstetric and surgical aspects of managing the patient with an abnormally invasive placenta (accreta / increta / percreta). Please join us, listen to our conversation on the podcast and let us know if you have any comments or questions.
Definitions:
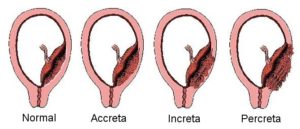
Accreta = the chorionic villi are in contact with the myometrium (78%)
Increta = the chorionic villi invade the myometrium. (17%)
Percreta = the chorionic villi penetrate the uterine serosa. (5%)
Risk factors:
- Previous caesarean delivery: The authors of one study found that in the presence of a placenta previa, the risk of placenta accreta was 3%, 11%, 40%, 61%, and 67% for the first, second, third, fourth, and fifth or greater repeat cesarean deliveries, respectively.
- Placenta previa (without previous uterine surgery): 1–5% risk of placenta accreta.
- Any condition resulting in myometrial tissue damage followed by a secondary collagen repair, eg myomectomy, vigorous curettage resulting in Asherman syndrome, submucous leiomyomas, thermal ablation , and uterine artery embolization.
ACOG
RANZCOG
Diagnosis – Imaging Modalities:
https://radiopaedia.org/articles/placenta-accreta
USS or MRI
Surgical management
Surgical management of placenta accreta: to leave or remove the placenta?
A Perez-Delboy, JD Wright 2014
Timing of Delivery
Placenta Accreta: When is the optimal time to deliver?
Manual Aortic Occlusion
Our podcast discussion on this topic
Interventional Radiology
3) REBOA during unexpected uterine rupture
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5628233/
2) Comment urging caution before embracing interventional radiology techniques:
http://www.obstetanesthesia.com/article/S0959-289X(16)30075-9/pdf
Communication and Having an Effective Team
Fostering a culture of safety: The OR team huddle
Conservative Management
Leaving the placenta in situ, Methotrexate, En bloc resection, Hysteroscopic resection