
Podcast: Play in new window | Download (Duration: 52:53 — 48.4MB)
Subscribe: Apple Podcasts | RSS | More
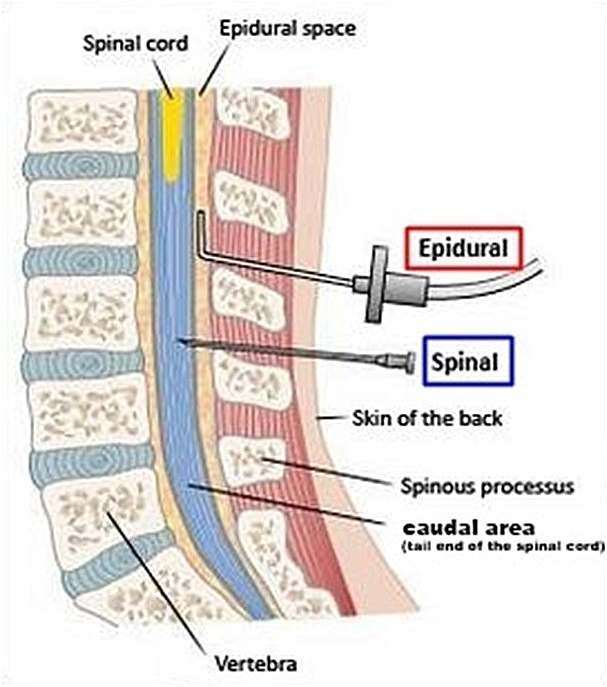
Your patient arrives in the anaesthetic room next to theatre, she’s booked for a non elective caesarean for failure to progress. She has an epidural in situ and you decide try to top it up – however after 25ml of lignocaine 2% with adrenaline and around 20min of waiting the block is stuck at the umbilicus and she can still move her legs relatively freely. This is obviously not going to be adequate – she is adamant she wants to be awake to see her baby born. You sit her up, pull out the epidural and do a single shot spinal with 2.1ml of heavy bupivacaine 0.5% + fentanyl 15mcg – after all you don’t want this block to fail as well!
You clean her back, lie her down and turn to talk to the midwife. When you turn back to the patient 30s later she looks a little purple and isn’t breathing…….
Hi everyone join Graeme and I this week as we discuss total spinal anaesthesia – a fascinating but somewhat scary rare emergency which can occur when we use regional anaesthesia in obstetric practice.
A big shout out to the team from Rotunda Hospital in Dublin who wrote the recent narrative review published in IJOA on this topic!
References
- Total spinal anaesthesia following obstetric neuraxial blockade: a narrative review Radwan, M.A. et al.International Journal of Obstetric Anesthesia, Volume 59, 104208
- Sobhy S, Zamora J, Dharmarajah K, Arroyo-Manzano D, Wilson M, Navaratnarajah R, Coomarasamy A, Khan KS, Thangaratinam S. Anaesthesia-related maternal mortality in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Glob Health. 2016 May;4(5):e320-7. doi: 10.1016/S2214-109X(16)30003-1. PMID: 27102195.